

I found this chart on reddit some time ago, I thought to repost it here as well
Pretty strange considering fluoxetine makes me sleep waayyy too much
Where is a living wage? That shit really helped me.
There’s no section for “brain zaps”.
I suffer from persistent depressive disorder with occasional major depressive episodes (aka “double depression”). These are just some notes in case anyone can relate. I also just find this kind of thing interesting…
- Bupropion (300mg qd for ~1-1.5 yrs): I felt no difference at all in my energy/interest levels, but also no noticeable negative effects.
- Diazepam (5-10mg prn): Barely perceptible effect at 5mg but felt slightly intoxicated at 10mg. Sometimes helpful to break out of dissociation during double-depressive episodes.
- Duloxetine (60-90mg qd for ~9 months): I felt no noticeable positive effects - only anorgasmia, insomnia, and restless leg syndrome the night of dosage adjustments.
- Escitalopram (10mg qd for 3-4 months): made me feel nauseous for ~30s every day without fail, and made me feel completely grey - no positive or negative feelings whatsoever.
- Trazedone (25mg prn): Effective for me as a sleep aid; no experience with chronic use as an antidepressant.
I did a bit of searching but I don’t really understand what QTc prolongation is. Can anyone help me understand?
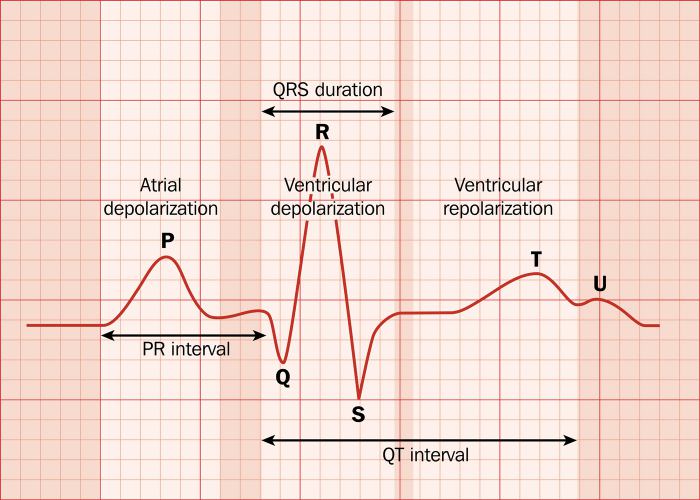
During your heart’s electrical conduction there are different phases. You have the contraction of the atria. The little pumps above the ventricle (main pumps) whose role is to help fill up the ventricles. The contraction of the ventricles. The main pumping part of your heart that pumps the blood to both your body and your lungs. And the repolarisation of both the atria and the ventricles. Basically the heart muscle reseting for another beat.
The atria contract first and repolarise first. On an ECG (heart trace) the atrial contraction corresponds to the P-wave. The little wave at the front. The atrial repolarisation occurs during ventricular contraction so you can see it on the ecg. When the ventricular contraction occurs you see the sharp up and down squiggles on the ECG. This is the QRS complex. Following ventricular contraction there is ventricular repolarisation. This occurs after the QRS complex and looks like a really big P-wave. This is the T-wave.
QTc prolongation is when the T wave takes a long time to occur after the QRS complex. When it gets too bad it is dangerous because the electrical energy that occurs in the T wave can set off another contraction of the heart. This contraction occurs outside of the normal pattern of the heart and the heart does not pump effectively leading to something called torsades de pointe which can develop into ventricular fibrillation leading to cardiac arrest (your heart not really pumping any blood).
Here is a labeled picture of an ECG ignore the u-wave its not really relevant and does not always occur.
Here is a picture of the heart showing the location of the atria and ventricular Heart
Thank you, that’s really helpful
https://en.m.wikipedia.org/wiki/QT_interval
The QT interval is a measurement made on an electrocardiogram used to assess some of the electrical properties of the heart. (…) An abnormally long or abnormally short QT interval is associated with an increased risk of developing abnormal heart rhythms and sudden cardiac death.
QTc stands for QT corrected for heart rate, the medication that increases QTc will increase the risk of certain dangerous heart conditions.
Thank you 😊
Escitalopram and Trazodone here. Out like a light on the latter. Only way I can function.
I’m glad Buproprion has few side effects from this chart.
However, for those considering it, here’s some missing side effects:
- Can increase libido. (A lot.)
- Can reduce weight. (A lot.)
- Can reduce your appetite/eating. (A lot.)
I’m not saying these are pros or cons. Each person should assess how these side effects will affect their own situation.
Needs a column for “makes you feel like you are Being John Malkoviching as you linger behind your own eyes and watch another version of yourself interact with the world while being confused about who is actually controlling your vessel”, and put Bupropion at a 12.
I have never been diagnosed with anything and never consumed any antidepressant or other psychopharmaceutical, but I get what you are describing like a lot, especially lately but since practically forever, at least since I was 12.
I practically often feel like the 2 taxi drivers in the Hudsucker Proxy (as I identify 2 internal voices) describing, in a detached way, whatever I do, including me typing on the keyboard right now (with one of them making fun of the fact that I still haven’t got the confidence to never look at the keys while typing).
Are we talking here about something that would hinder me functioning socially and professionally or does what I described count towards something I should take care of?
That… explains a lot about a few months of my life
That shit is trippy as fuck to me, and not in a good way. More of a Twilight Zone sorta way.
I took Bupropion exactly once, and that day happened to coincide with the day of a first date. There was not a second date. I’d say something to her, but it wasn’t me, it was the “me” who was standing about three feet in front of me. I swear to Cotton Eyed Joe I could see the back of my own fucking head.
I didn’t get it nearly that acutely, but I made several stereotypical “crazy person sketches” of my view through my glasses with all the visible objects being written words instead of objects, trying to convey how lifeless and disconnected I felt from my own sensory input
a few years later I learned that’s called “dissociation” and it’s not supposed to happen 🫠
Seems to be missing the entire MAOI class (moclobemide, selegiline, phenelzine, tranylcypromine, isocarboxazid), and most tricyclics (clomipramine, imipramine, nortriptyline)
Had a doctor tell me I should never feel the antidepressant. Should be a background thing. Thought that was good advice.
Setraline leveled me the fuck out.
It’s kinda funny how much medicines’ effects can vary from person to person, I tried sertraline and had absolutely no difference, whereas my mother and my sister take it and it works for them
May I ask, what do you mean it leveled you out?
Anger flare ups stemming from depression. Took cognitive behavioral therapy for a time until I could learn the coping skills. Still take the setraline.
Have noticed when I wheen off/am off it am more prone to those flare ups. They don’t happen outright, I just notice them more prominently.
I tried many of those with no success, until tried Duloxetine and the response was optimal. Each persons has different reactions.
If y’all have had really bad side-effects look into pharmacogenomic testing, it can help rule out bad medicines before you try them
I had one done a while ago and it marked a ton of medicines that I had already tried, (and had bad effects from) and a bunch I hadn’t tried yet. Since then, I’ve had much fewer bad experiences
notes
-
the one I did had a specific brand name but I don’t remember what it was. (It was a while ago) I’m pretty sure this is what it was though
-
you might have to remind your doctor about it when they’re prescribing medications, this still isn’t very well known afaik
-
this isn’t sponsored/paid/other bullshit, this is an actual recommendation (though I felt like one of those ‘ask your doctor if !@#$ is right for you’ american commercials the entire time writing it)
I also had testing for psychiatric medication-gene interaction, and can recommend it as worth it (and am in the US)
-
My wife tried fluoxetine (Prozac), and it really impacted her libido and weight gain. She was also very drowsy, but that’s not listed. She’s now on bupropion (Wellbutrin) and is just living her best life. We were late 20’s when she started taking it so the libido impact is super important to us. The biggest thing she says about Wellbutrin is that it can cause a little irritability with alcohol, and she’s glad she didn’t start that at the same time as adderall since it’s kinda the same.
An off label use for Trazadone is as a sleep aid. At doses under 150 mg it doesn’t really work as an antidepressant but will make you drowsy. I’ve been prescribed it before as the first step before Ambien
Amitriptyline as well, started taking it for peripheral neuropathy. Ended up on a higher dose because it’s a heavy sedative. Take it before bed, and I’m out. I was taking Zopiclone before, to help me sleep but don’t need it now. Also it failed as an antidepressant but works wonders for antianxiety.
We have it for our dog. We got it first when she was spayed and needed to chill out in order to not rip stitches and now we have it to give before stressful situations (guests, vet, etc). It definitely makes her more tired, but she will still fight through it to be crazy.
I thought it’s use as an antidepressant was completely discontinued because of that.
¯\_(ツ)_/¯
I’m not a doctor, just need help sleeping sometimes
Can confirm, bupropion causes insomnia.
I sometimes have to take nighttime benadryl to help me sleep.
Been on it consistently for over a decade now and have always been funky with sleep. I started back in undergrad when the pressure of life left me spiralling out of control, and have since always thought I was just a weird sleeper.
I have insomnia semi often, usually anxiety-induced, but I’ve never thought that it could be the bupropion directly.
Very curious, and good to know.










{kind=link}
{kind=link}
{kind=link}